NYAPRS Note: Psychiatric advance directives can play a crucial role in ensuring that effective and engaging care is delivered to people with the most extensive mental health and substance use related conditions, especially during times of major crisis.
PADs give healthcare professionals the best information and direction available as to how to deliver the best crisis support from the best informants of all, the individuals themselves. They operate from the place of informed choice, as a powerful alternative to coercive approaches that could otherwise deliver care in an uninformed and potentially inappropriate or harmful manner that would discourage people to stay connected with services after the crisis.
The following piece provides details of specific successful examples of how PADs are being used. Note below how federal agencies like CMS are raising expectations that hospitals look for PADs and SAMHSA is developing strategies to promote their greater use.
Up to now, PADs are rarely understood or being used….yet their insertion into electronic healthcare records could make their use common someday soon.
See more about PADs at https://www.nrc-pad.org/ and contact our NYAPRS Training Collective at ruthcw@nyaprs.org to schedule a PAD training in your area.
Now Mental Health Patients Can Specify Their Care Before Hallucinations and Voices Overwhelm Them
Psychiatric advance directives allow patients with serious mental illness to specify the treatment they want if they become too sick to say so.
By Pam Belluck New York Times December 3, 2018
CHARLOTTE, N.C. — Steve Singer, who has bipolar and borderline personality disorders, knows when he’s on the verge of a mental health crisis. The female voice he hears incessantly in his head suddenly shuts up, and the hula hoop he gyrates while walking to the grocery store stops easing his anxieties.
That’s when he gets to a hospital. Usually, talking briefly with a nurse or social worker calms him enough to return home. But this year a hospital placed him on a locked ward, took his phone, and had an armed guard watch him for 20 hours before a social worker spoke with him and released him.
“I get the heebie-jeebies thinking about it,” said Mr. Singer, 60. “They didn’t help me, they hurt me.”
Deeply upset, he turned to something he’d never known existed: He completed a psychiatric advance directive, a legal document declaring what treatment he does and doesn’t want. Increasingly, patients, advocates and doctors believe such directives (called PADs) could help transform the mental health system by allowing patients to shape their care even when they lose touch with reality. Hospitals must put them in patients’ medical records and doctors are expected to follow them unless they document that specific preferences aren’t in the patients’ best medical interest.
As the pendulum has swung from institutionalization to outpatient care, psychiatric directives also offer a middle path by allowing patients to designate family members to speak for them when they’re too sick to do so themselves.
But some doctors and hospitals are wary that the documents could tie their hands and discourage treatment they consider warranted. Some worry the directives won’t be updated to reflect medical advances. Others question whether people with serious psychiatric conditions are ever capable of lucidly completing such directives.
“A decision based on erroneous information on a PAD, that can happen,” said Dr. Katayoun Tabrizi, a forensic psychiatrist at Duke. “This is not a cookbook.”
Still, early research and experience suggest that PADs, authorized by law in 27 states and possible in others as part of conventional medical advance directives, could help some of the millions of people with serious mental illness cope better and guide doctors treating them.
“PADs could be a very important tool to minimize hospitalization and minimize involuntary commitment,” said Cherene Allen-Caraco, chief executive officer of Promise Resource Network, a peer-counseling organization in Charlotte. By letting patients give permission beforehand to be committed to hospitals they prefer, the directives can avoid the arduous court-ordered commitment process — traumatic for patients, especially if they’re handcuffed by police.
“And by listing what’s been hurtful to you in the past and what’s been helpful to you, that could be an advantage to the treatment provider,” Ms. Allen-Caraco said.
As people with serious mental illness cycle in and out of hospitals, many landing on the streets or in prison, better approaches are urgently needed.
Now, there are growing efforts to train counselors to help patients complete PADs and urge hospitals to honor them. The federal Centers for Medicare and Medicaid Services has strengthened requirements that hospitals ask if patients have advance directives, including psychiatric ones. The federal Substance Abuse and Mental Health Services Administration is considering ways to encourage directives. And PAD-completion clinics are emerging in Texas, North Carolina and elsewhere.
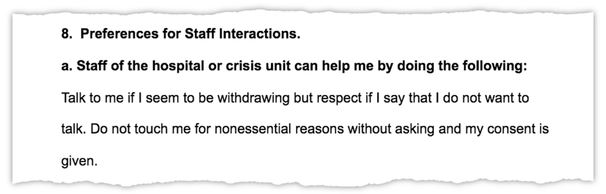
In the documents, patients specify treatments they like or despise; whether their crises involve suicidal feelings or hallucinations; even how to treat their service dogs and what doctors should say to penetrate their psychoses. Some patients carry copies, share them with relatives and their regular psychiatrists, and, when possible, register them in state databases.
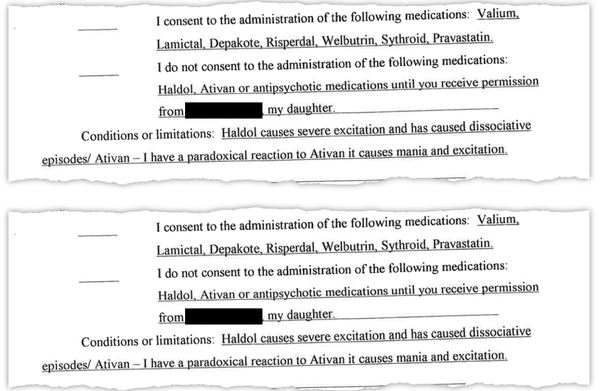
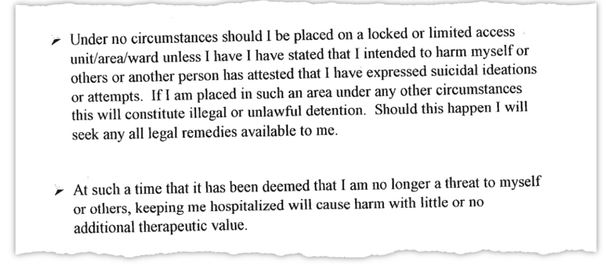
Mr. Singer’s lists his preferred hospital, five psychiatric medications he’ll accept and two he won’t because they make him excitable. It says he rejects electroconvulsive shock therapy and refuses to be on a locked ward unless he or a trusted person says he intends to harm himself or others.
Dr. Marvin Swartz, a Duke psychiatry professor, said simply writing a directive increases some patients’ engagement in treatment, reducing setbacks with medication and therapy. After he and colleagues offered 239 patients the opportunity to complete PADs, they found the 147 who did so had fewer crises that led to being involuntarily hospitalized, medicated or restrained.
Mr. Singer, a former X-ray technician, knows he sometimes needs inpatient hospitalization. He’s tried to kill himself three times: at 15 by hanging himself from a shower rod (it broke); in his 40s with his father’s World War II pistol (it jammed); and in 2012 with a shotgun (a pellet grazed his scalp and punctured the ceiling). After that attempt, he said he told a hospital, “‘It was my Walmart shotgun or to you guys. I need somebody to put me behind a locked door.’”
Usually, though, he recognizes early symptoms, like his impulsive five-hour drive to a Johnny Appleseed statue in Virginia or a broken keychain that panicked him into thinking: “I’m going to lose my keys and get evicted and a meteor is going to strike,” he said. “You’ve heard of catastrophic thinking?
That’s for amateurs. I have apocalyptic thinking.”
While briefly visiting a hospital stabilizes him, being confined there worsens his anxiety, he said. “I don’t need anything that is going to move me one milli-scintilla in the shotgun direction and being locked up did a whole lot more than one milli-scintilla.”
His directive lessens his concerns about seeking hospital help. On a chocolate-colored couch in his apartment, Mr. Singer, wearing an Alice-in-Wonderland T-shirt, said he’s been taking medication regularly and forgoing recreational drugs like mushrooms. “That psychiatric advance directive, I think is so important,” he said. “It allows me to turn things around.”
Family can help
Ariel Wolf, 25, has been hospitalized 30 times since she was 13. She believes her PAD helped her get treatment that worked.
Ariel Wolf, 25, has been hospitalized over 30 times since age 13, when she began cutting herself with razor blades. Her brain directed her to inflict injuries meeting “certain dimensions of width and depth and location on my body,” she said recently in a cafe near her home in Winston-Salem, accompanied by her service dog, Jubilee.
She’d slash her arms, elbows, shoulders and feet, photographing the wounds and sewing them up with fishing line. “By the time I got to 5,000, I was sitting in the bathroom all night, obsessively cutting,” she said. At 15, aiming to remove her appendix, she sliced a three-inch gash, stopping only when her mother came home.
At 17, during months of psychiatric hospitalization, Ms. Wolf, who has bipolar disorder with psychotic features, swallowed staples and shoved a paper clip into her thumb. But just before her birthday, she completed a directive, allowing her parents to participate in her care after she turned 18.
That helped save her, she said. Her parents communicated her directive’s preferences, including objections to electroconvulsive therapy and antipsychotic medications. Before having the document, she believes doctors sometimes considered her obstinate and forced treatment on her.
Even skeptics of PADs value that they let patients pre-authorize involvement of family or friends. In crises, patients might be too unstable or paranoid to give permission, said Victor Armstrong, a vice president for Atrium Health who runs Behavioral Health Charlotte, a 66-bed psychiatric facility.
Ms. Wolf, now a mental health peer support specialist, said she no longer self-harms, but needs occasional hospitalization when experiencing symptoms like speaking in rhymes or hallucinating that light is stabbing her. Her recently revised directive indicates her parents aren’t needed as medical guardians but should be contacted. Its additional details include: “I have a history of experiencing mania/hypomania in or around March, August, and sometimes November.”
Obstacles to overcome
For PADs to become widespread, major logistical hurdles remain. Although hospitals are technically required to ask whether patients have advance directives, psychiatric directives aren’t yet common enough for hospitals to routinely embrace them. Until then, some patients won’t complete them, “a chicken and egg problem,” Dr. Swartz said.
Mr. Armstrong called PADs “a wonderful notion” that his hospital would try to follow, although they wouldn’t supersede doctors’ judgment or “override their fear of being sued.”
Completing them requires detailed steps. In Charlotte, Judy Reiner said that because her 45-year-old son didn’t get his directive notarized, it wasn’t valid during a recent crisis and he endured involuntary commitment.
Many patients need extensive help writing directives, but proponents say psychiatrists and relatives shouldn’t assume that role because patients may suspect they just want to make hospitalization easier.
Effective PADs “would enhance people receiving appropriate treatment,” said Dr. Mark Rapaport, chairman of psychiatry and behavioral sciences at Emory University. “But this is going to be really hard to do.”
Ms. Allen-Caraco of Promise Resource Network, whose psychiatric diagnoses include major depressive disorder, said some patients are “afraid of legal documents because they have been associated with removal of rights.” At a PAD clinic, she provided helpers, witnesses, a notary and assistance registering PADs in the state database.
At the clinic, Bebe Smith, a clinical social worker, encouraged patients to be specific, but realistic: “If you say, ‘I want to have milkshakes every day,’ that’s not a standard treatment.”
She helped Lashawanda Ivey, who has schizoaffective and borderline personality disorders, complete a PAD. Ms. Ivey trembled as she recalled requesting hospitalization recently because “ voices in my head were louder, and suicidal thoughts were coming.” The hospitalization turned into “an excruciating two days because people weren’t really listening to what I was saying.”
Her PAD says hospitals shouldn’t “overload me with a whole lot of questions” and that although she dislikes electroconvulsive shock, it’s helped her become communicative, so “if they have to do it, yeah.”
In another room, Harrison Pedigo, 26, got his directive witnessed and notarized. He wrote it in 2016, after four hospitalizations, beginning when his parents had him involuntarily committed because he was babbling, smearing paint on the carpet and walking barefoot in traffic. He said he hallucinated while hospitalized, including imagining he was telepathically communicating with a man wearing playing cards.
His PAD objects to three drugs and one hospital, and allows his parents’ involvement, preventing a recurrence of the time a hospital wouldn’t confirm he was there when his mother brought him clothes.
Since completing it, he hasn’t been hospitalized. He takes voice-over classes and lives with his parents in a townhouse decorated with his colorful abstract paintings. His directive is “a safety net,” he said, “to help something not happen again or go smoother if it does.”
Harrison Pedigo, at home with his parents, Leigh and Paul, suffers from schizophrenia and drafted a PAD in 2016 after four hospitalizations.CreditTravis Dove for The New York Times
A window into the human psyche
PADs can be Rosetta stones to a patient’s inner life.
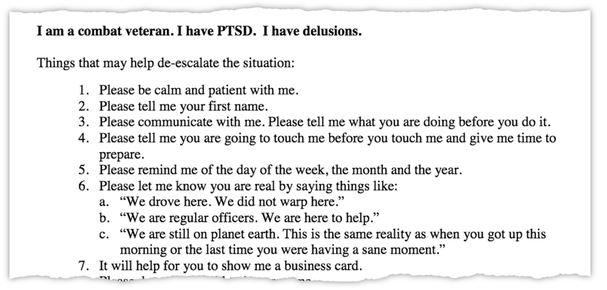
“Sometimes I hear voices that seem to come from another person’s brain,” Andrew, a 29-year-old military veteran from Houston, wrote in his directive’s 18 remarkably frank pages. “I may find it helpful to think about obscure movies other people have probably not seen.”
He listed 15 things that help deter him from quieting his demons with illegal drugs, including origami and playing catch. Conversation is good, wrote Andrew, who asked that his last name be withheld to protect family privacy. “But,” he cautioned, “it is very important that the attempt to converse does not include good-natured jesting, joking or hazing.”
“Sometimes I think that people are not who they say they are,” he advised. “Please let me know you are real by saying things like: ‘We drove here. We did not warp here.’”
Laurie Hallmark, managing attorney for mental health programs at Texas RioGrande Legal Aid, who helped Andrew draft his directive, said that recently, when he was hospitalized and completely inside psychosis,” a nurse followed his PAD, essentially saying “‘Oh wow! I recognize these behaviors.’” ”
Andrew’s directive includes small steps to defuse big crises.
“Things that may help me to not want to kill myself,” Andrew listed. Among them: drinking Yogi tea and discussing a concept called “infinite replay” — although he added, “I understand that other people may not find this topic fascinating.”
In emergencies, before hospitals use medications, seclusion or restraint, Andrew implores them to try other approaches.
“Please,” he wrote, describing one, “say ‘It’s going to be ok.’”
https://www.nytimes.com/2018/12/03/health/psychiatric-advanced-directives.html