Why Our Approach to Suicide Prevention Needs to Change Now
by Leah Harris Mother, survivor, storyteller, mental health advocate
Huffington Post September 24, 2015
I write about suicide prevention as an advocate, but also as a suicide attempt survivor myself. I first entered the mental health system after an attempt in adolescence, the first of several efforts to end my life. My hospitalizations felt more like punishment than care. I frequently witnessed distressed children being restrained by adults for “acting out,” which terrified and traumatized me. (I later learned that teens have died during such “take-downs” in psychiatric hospitals.) Upon intake and discharge, professionals dutifully made me sign “no-harm contracts,” but there was little to no follow-up, and I was never supported in the community to find reasons to live.
This is National Suicide Prevention Awareness Month, and the suicide prevention world should be very uncomfortable. The latest available data show that 2013 marked the tenth year in a row of increasing suicide rates in America.
Despite all the hearts, minds, and good intentions being poured into suicide prevention, the prevailing strategies don’t seem to be working.
In 2014, I attended a research progress meeting at the National Institute of Mental Health (NIMH), where former NIMH director Dr. Thomas Insel shared what he called an “inconvenient truth.” He showed a graph comparing mortality from stroke, heart disease, AIDS, and leukemia from 1990 to 2010. In every single case, there have been impressive decreases in mortality over this time period. The steady decrease in mortality stops when we come to rates of suicide.
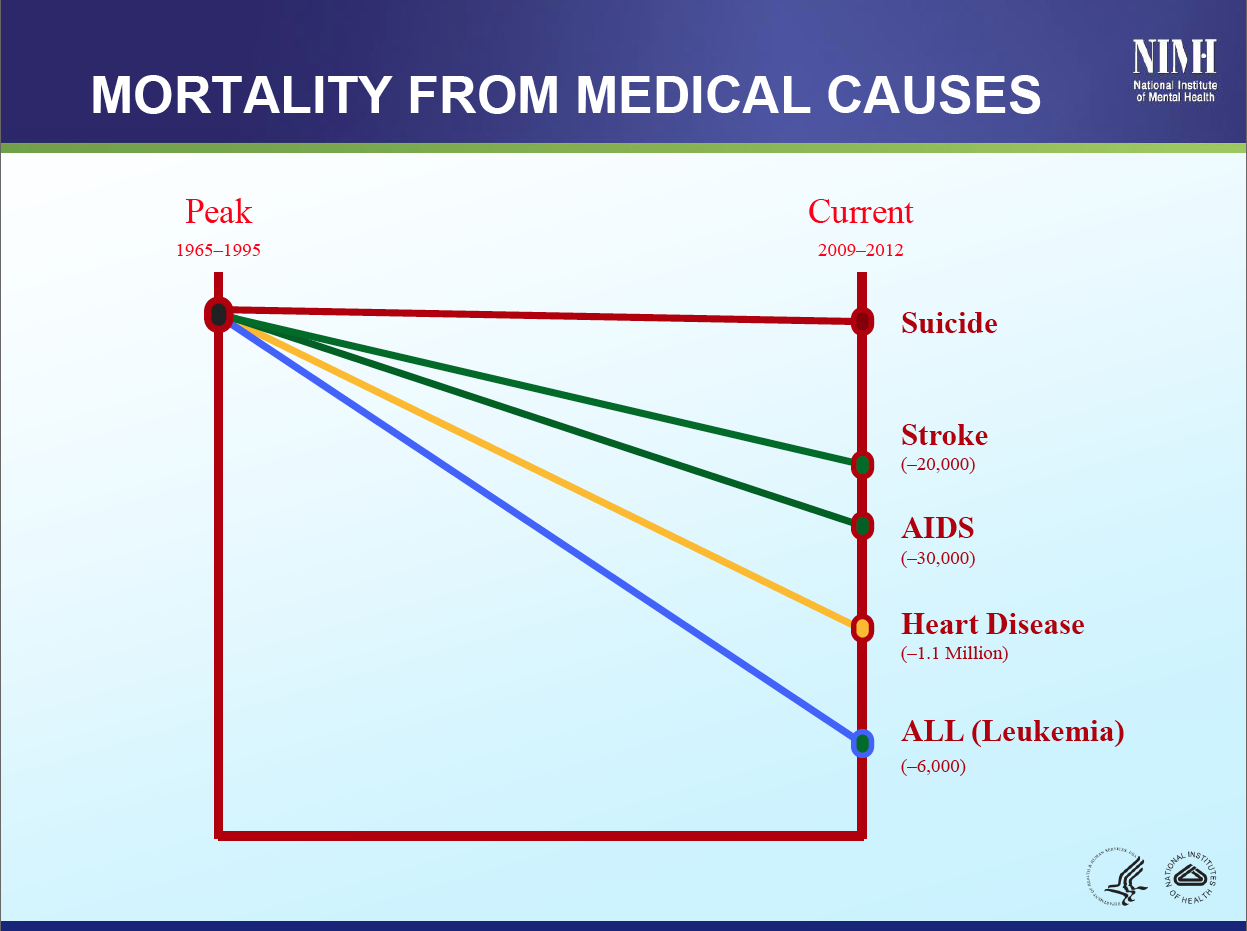{kind=link}
Is this “inconvenient truth” simply explained by a lack of investment in suicide prevention, as many in the field might argue? Certainly, this is part of the problem. Compared to other leading causes of death, suicide receives a relative dearth of funding. Suicide is the tenth leading cause of death in America, and the third leading cause of death in youth, yet we withhold precious resources that could be devoted to reducing mortality.
But the problem is much deeper than that. The primary goals of most suicide prevention efforts are to teach the public to “recognize the signs” of suicide and refer the person to get appropriate help. But what will this help actually look like, if or when it arrives? All too often, the kind of help people receive, if they can access help at all, can hurt more than it helps. A recent expose in the New York Times explained how one battalion, fed up with the lack of quality care and support from the Veterans Administration (VA), has created their own social network to support one another to stay alive another day.
These veterans may be on the right track. Research indicates that access to “help” may actually contribute to increased suicide risk. A recent study published in Social Psychiatry and Psychiatric Epidemiology found that the more intensive contacts that people had with mental health treatment, including inpatient hospitalization and contact with emergency rooms, the more likely they were to attempt or to die by suicide. The Suicide Prevention Resource Center (SPRC) also published an in-depth document examining this phenomenon of increased risk of suicide after discharge from inpatient services.
The implications of these findings are astounding, yet the general public is largely unaware: the treatment we have on offer may be making things worse. When you couple this sobering reality with the fact that the training most mental health professionals receive in suicide prevention is “woefully inadequate,” then you have a recipe for the disaster we currently face.
On top of poor treatment in the mental health system, we have criminalized suicidal behavior by designating law enforcement as first responders. Friends, family, and even suicide hotline workers often feel they have no choice but to call 911 on people who are actively suicidal. I can attest from personal experience that being carted away in handcuffs and put in the back of a police car after a suicide attempt was anything but therapeutic. And on far too many tragic occasions, when loved ones call 911 for help for their suicidal family members, the police show up and “finish the job” if the person resists being taken away. We then call it “suicide by cop,” essentially blaming the victims for their own deaths. Clearly, our collective responses to suicidal behavior, which are largely based on fear and ignorance, have the effect of re-traumatizing already traumatized people.
One thing we know about suicide, but which is rarely reflected in research or practice in the suicide prevention world, is the high prevalence of trauma and adverse childhood experiences (ACEs) among suicidal people. Researchers found that ACEs were a factor in nearly two-thirds (64%) of suicide attempts among adults and 80% of suicide attempts during childhood/adolescence. The more ACEs one has, the more likely they are to attempt suicide. It makes sense then, if we’d like to reduce the prevalence of suicide, that we focus on preventing childhood and adult trauma, and ensuring that people receive care and support that does not create further trauma and pain.
There is some reason to hope that trauma will begin to be taken more seriously by health care providers serving suicidal people. Zero Suicide, a national training and technical assistance initiative, is encouraging health care systems to practice trauma-informed approaches as part of their overall efforts to reduce deaths by suicide.
We also could do much to prevent suicide by enacting sensible gun reform. In this country, significantly more people die from suicide by firearm than they do by homicide. Suicide is often an impulsive act, borne of moments of extreme despair. But few people will survive a bullet if they have easy access to a gun. There is a clear relationship between gun ownership rates and suicide rates: more guns equals more suicides.
While “means reduction” is a hot topic in suicide prevention, most mental health professionals are not trained sufficiently to ask their clients about guns. And according to a 2013 publication by the Harvard T.H. Chan School of Public Health, “people contemplating gun suicide are not always in treatment and often don’t display clues in advance–not even to themselves.” While it may be politically unpopular, we need policy-related advocacy from suicide prevention advocates towards changing the obscenely lax gun laws in this country.
The suicide prevention field should also be addressing the shocking lack of community support for suicidal people.
The Centers for Disease Control and Prevention (CDC) cite community connectedness as a central protective factor against both suicide and interpersonal violence. If you have lost a loved one to suicide, there is generally a support group near you where you can connect with others and begin to heal. But if you have survived a suicide attempt, and have just been discharged from the hospital, there is likely no peer-to-peer support group for you in the community.
Grappling with suicidal feelings, or surviving an attempt, are immensely confusing and difficult experiences to discuss, even with well-meaning family and friends. Having the opportunity to share these experiences with others who truly “get it” can make all the difference.
There are some positive changes on this front, as well. The Western Massachusetts Recovery Learning Community has successfully run peer-to-peer Alternatives to Suicide groups for years, and they offer training and consultation to other communities wishing to start such groups in their area. Didi Hirsch Mental Health Services has also created a manual for a similar purpose. These efforts give me hope that we can anticipate more community support to help people who are suicidal to discover a life worth living.
We must shift the paradigm on how we understand and respond to suicide. Now is the time to think further out of the box than we ever have before. We must stop doing the same thing, year after year, and expecting different results. This is the very definition of insanity. If we do not drastically change course on our suicide prevention strategies, we will keep having these National Suicide Prevention Weeks and National Suicide Prevention Awareness Months and fundraising walks into the darkness year after year, as the suicide rates continue to climb.
___________________
If you — or someone you know — need help, please call 1-800-273-8255 for theNational Suicide Prevention Lifeline. If you are outside of the U.S., please visit the International Association for Suicide Prevention for a database of international resources.
Follow Leah Harris on Twitter: www.twitter.com/leahida